
A new operating model for health and care
Delivering the system’s core objective: the left shift
Moving the money to earlier, more cost-effective interventions should improve allocative efficiency, boosting productivity to help address the NHS financial challenges (alongside ongoing efforts to improve technical efficiency). This will require “hardwiring of financial flows”
through three levers:
- Payment mechanisms: A payment mechanism – adopted in the NHS Payment Scheme from April 2026 – which incentivises earlier, proactive intervention. This is likely either an outcome-based contract or capitated contract, where providers keep any savings from allocative efficiency.
- Gain/loss share mechanism: All providers along a care pathway must have an aligned financial incentive to deliver care earlier and avoid downstream admissions, ensuring acute providers are not financially penalised for doing so. This will likely be through a lead/integrated care provider or partnership, which sub-contracts services.
- Measurement: If the objective is to move money into primary and community-based care, we must know whether it is being achieved. This will require a metric which is monitored locally and nationally and enables intervention when necessary.
Rather than promoting one delivery model, the centre should create strong incentives for systems and providers to develop a credible collaboration and accountability model that suits their local legacy and assets. The centre should require business plans and medium-term financial plans backed up by clinical plans defining care transformation (in particular around elective care). Monitoring progress in delivering the left shift will allow the efficacy of different models to be assessed and, if necessary, adapted.
Different delivery models
Integration and transformation are being delivered differently across systems. As each ICS is different, enforcement of a uniform approach to delivering the left shift would not work and risks creating unnecessary expense, significant disruption and delaying delivery. To deliver reform, practical, responsive and inclusive governance arrangements are needed to solidify partnership working as the expected standard at the heart of commissioning and delivering quality care.
Clinical leadership will be key to delivering transformation, as will building consensus between clinical and managerial staff. Appropriate local arrangements should evolve from a robust understanding of system context and commitment to shared principles, generating a partnership structure that is greater than the sum of its parts and maximises the strengths of each unique organisation or contributor. There is a precedent for different approaches to this, as outlined below.
The focus of any delivery model should be on delivering a person-centered and outcome-focused approach. Local leaders should be empowered to elevate where things are best delivered at scale and held accountable for the outcomes they achieve – not for developing a particular structure.
Within every model, partnership at place level – at a population size of around 250,000-500,000 – will be critical to moving towards more integrated, person-centred care and optimising the use of collective resources. Since the integration white paper and Thriving Places guidance, place partnerships have been the expected delivery model in England. [26],[27] Systems such as Cambridgeshire and Peterborough have a vertical model in which the ICB contracts with each place, potentially delegating commissioning responsibilities and/or financial allocations and a provider or provider collaborative is usually the designated ‘lead’ for integrating care. Leeds is another example of a place-based approach, where budgets are pooled across NHS bodies and local authorities. At this more local geography, commissioning can be integrated with co-terminous local authorities and proactive care can be planned around populations.
In other systems, particularly smaller systems such as Gloucestershire, where there are just two providers, there is a distributed model of leadership. This model may become less common with ICSs becoming larger and fewer in number. [28]
In other systems, the budget is delegated to a lead provider which then sub-commissions services to be delivered at place or neighbourhood level. For example, in Birmingham and Northumbria, a provider is designated to lead the commissioning of services, with delivery devolved to local neighbourhoods. In other systems, like Hertfordshire and West Essex ICS, the primary care at-scale provider is the lead provider of an integrated urgent treatment centre, which they deliver as part of a collaborative with other community, acute and out-of-hospital providers.
These provider collaborative or lead provider models may form the basis of an accountable care organisation (ACO) type approach – a provider with delegated responsibility for improving the health of a particular population cohort and planning the most cost-effective care interventions to that end. Through sub-contracting services, this approach ensures multiple providers across a care pathway have aligned incentives, sharing financial benefit from better managing demand and preventing more costly downstream interventions.
ACOs have precedence in other countries, including Spain, Germany and the USA, and despite proposing the idea in 2014, the Health and Care Act 2022 effectively moved England towards accountable care systems in the form of ICBs. [29]
However, the current approach does not align incentives across providers. The latest NHS operational planning guidance signaled a move towards lead providers being given responsibility for planning and transformation of local services for a defined population cohort, stepping in the ACO direction. [30] This would require devolving knowledge and skills to provider organisations. NHS England indicated that this may extend to delivering strategic commissioning directly (through delegation arrangements and provider collaboratives), but that an accountable care model would only be explored in the most mature systems. [31] It is therefore a delivery model that is unlikely to take precedence for at least a decade.
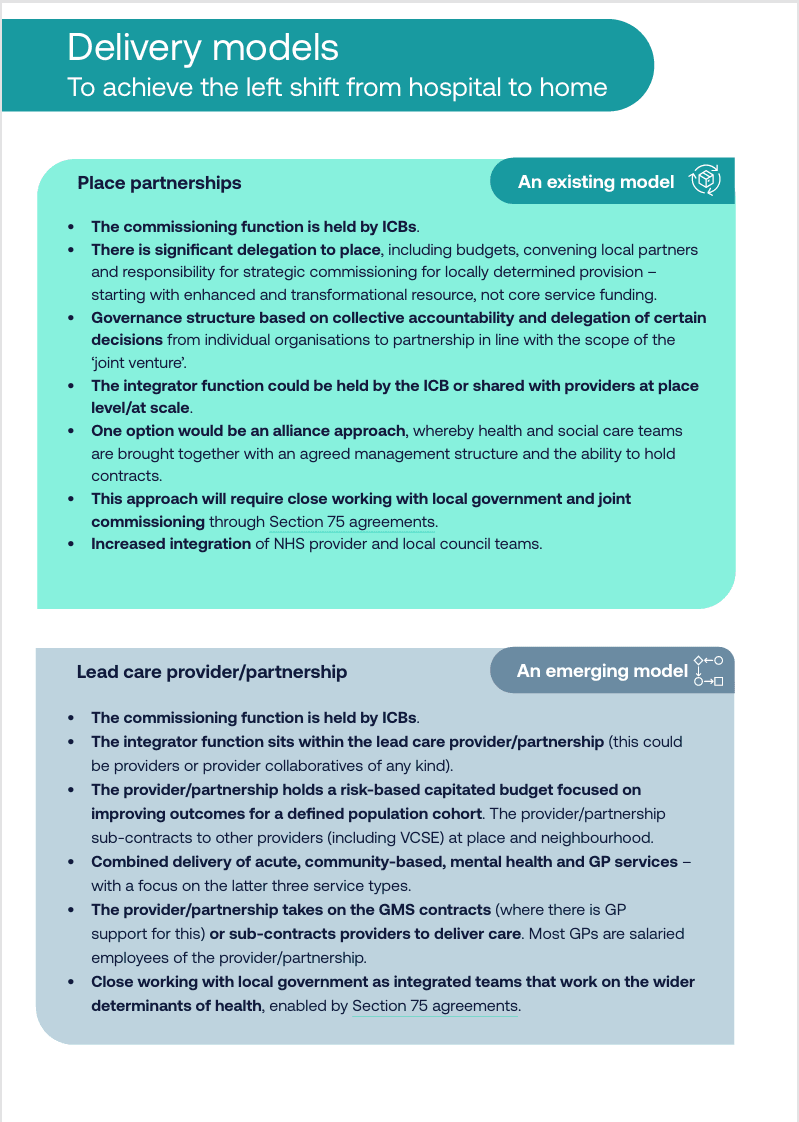
The below model illustrates three emerging ‘delivery models’ for achieving the left shift through place-based collaboration. These are archetypes which are presented to offer clarity. They and not mutually exclusive (for example, place could effectively be a lead provider) and are not intended as a definitive description of the future direction of travel.
Delivery models to achieve the left shift from hospital to home
Case study: Birmingham and Solihull Integrated Care System’s Community Care Collaborative (example of a community trust lead provider model)
The Community Care Collaborative is a partnership between primary (predominantly general practice), acute, community, mental health, social care and ambulance services, as well as the voluntary sector. It aims to provide better joined-up health and care services in local neighbourhoods across Birmingham and Solihull, making it easier for people to access the care they need closer to home and reduce pressure on local acute hospitals.
Its East Birmingham Locality Hub was the first launched in December 2023 and has been the trailblazer of this new and innovative approach to creating a neighbourhood health service at a locality level. Their approach integrates social prescribing, community care and key interventions, such as healthy lifestyle support, befriending and family and carer support, all coordinated by the multidisciplinary team. The hub, which also benefits from a co-located urgent treatment centre and community diagnostic centre, is particularly focused on improving care for people with high intensity use of emergency departments (locally known as frequent service users), by offering personalised support at the neighbourhood level.
In their first year the Community Care Collaborative have achieved:
- GP attendances – down 31 per cent
- A&E attendances – down 20 per cent
- Inpatient spells – down 21 per cent
- Outpatient spells – down 25 per cent
- Community contacts – down 15 per cent
Case study: ChenMed model of risk-capitation funding in the USA (example of a primary care lead provider model)
ChenMed operates under the MediCare Advantage model in the US and aims to create financial incentives to keep people well and out of hospital.
MediCare (the commissioner) gives ChenMed, a primary care and wellbeing provider (the lead provider), the budget to cover the cost of healthcare for a particular population cohort (people over 65 with complex health needs and/or high levels of deprivation). ChenMed have an incentive to keep people healthy (and make a profit on savings) through their services, but will sub-commission acute and other services when required.
Despite similar complex health needs among their patients, ChenMed averages 1,324 inpatient hospital days per 1,000 patients over 65 compared to an average of 2,220 across Miami and 2,236 in England. Read more about this model in Unlocking reform and financial sustainability.
Primary care at scale
For primary care to operate as a lead provider, it is imperative that primary care is supported to operate in an integrated way, carry risk and work at scale. Primary care leaders must be empowered to drive change as opposed to being ‘done to’. The government should therefore strongly incentivise the development of primary care provider collaboratives to bring together primary care providers at place/system level to have a collective voice and with the ability to become legal entities that can hold contracts and act as a strategic provider partner to the ICB and the rest of the system.
Primary care provider collaboratives are now developing across the country – many supported by the ICB to establish as a collaborative and become a legal entity that can hold contracts or be hosted by an existing legal entity. In areas where there are strong and mature federations, such as Herefordshire, the collaborative has been built around the federation infrastructure.
In other places such as Sutton, it is through an alliance of primary care networks and others, such as in Birmingham and Solihull, the collaborative (which brings together primary, community, mental health and social care) is hosted by the community trust. Collaboratives should embrace wider primary care – pharmacy particularly – given the opportunities to use their capacity and infrastructure, as well as optometry, dentistry and audiology.
To support integrated working, the workforce should be developed around multi-disciplinary teams that include GPs, nurses, social workers and mental health professionals. All health and care professionals working in these neighbourhood hubs should also have access to digitally enabled and integrated shared care records which would help improve the continuity of care and ensure services are patient-centred and responsive.