Beyond the waiting room: reimagining primary care for the next decade
The role of primary care in at-scale provision
Dr Nigel Fraser
Chair, Taurus Healthcare GP Federation
Introduction
The government has announced its three shifts – hospital to community, analogue to digital and sickness to prevention. These are sensible and desperately needed, as it has never been clearer that we cannot just continue as we are and expect different outcomes.
We do this at a time of unprecedented financial pressures and a health service struggling to recover in the aftermath of the pandemic, albeit five years down the line. Acute hospital funding has expanded considerably over the last five years, but funding for general practice has fallen in real terms (while demand rises). Lord Darzi acknowledged in his report that despite the strategy of investing in out-of-hospital care, we have done the opposite and, unsurprisingly, are not the better for it.
There is a clear opportunity to shape thinking in this space; now is not the time to fight for the status quo.
The centre will change, both in size and function; systems will be smaller and more focused on strategic commissioning; and there will be pressure for providers to look for new efficiencies. This gives a clear signal that the reform agenda has started, and a greater role will be needed from providers.
There does not appear to be a reluctance to adopt a radical approach to solving the major problems we are facing. The role of primary care in an increasingly integrated provider model is unclear and will depend on its appetite to be part of the solution. There is a clear opportunity to shape thinking in this space and now is not the time to fight for the status quo.
General practice
There is clear agreement that the foundation of general practice is the care delivered at practice level, which is indeed the ‘beating heart’ of NHS general practice and indeed the NHS. The value of continuity, for those who need it, and a longitudinal approach to care, brings the NHS immense value. This area has seen a squeeze in resources pushing practices to transform the delivery model and absorb massive real-time cuts. This has not been fair or warranted, but we may be seeing this addressed through the 2025/26 GP contract, that while not an answer, at least signals perhaps a turning point.
Primary care networks
PCNs have seen considerable investment since 2019, and with an average footprint of 30,000-50,000, allow practices to work together. While the profession remains divided on their success, there is no doubt they have provided a vehicle for GP leadership development, which is welcome. But we need to continue that journey.
GP federations and at-scale providers
Despite the role and value of federations and at-scale providers, there has been a piecemeal approach to their evolution despite them providing services that can be co-terminus with other place-based partners. There are a variety of models but where these have been successful, they have a strong governance link to membership practices and PCNs, so that the services are delivered in a truly integrated manner.
An example of this is out-of-hours provision that requires a larger footprint than PCNs and can benefit from integration with in-hours general practice. This only works when the consensus is that this is part of general practice and feels owned by general practices. This is not the case everywhere. When done successfully it can return 24/7 general practice services and enable risk and complexity to be managed out of hospital, including a more localised NHS 111 clinical assessment.
When these tiers are aligned, with the correct governance, each tier is supported by the others and general practice collectively is stronger. The other piece of the jigsaw is the vitally important role of the local medical committees that need to be involved as the statutory representatives of GPs. Getting this right is not easy and there are a variety of models where this has been enabled, such as in Cornwall; Berkshire, Buckinghamshire, Oxfordshire; and Herefordshire.
This adds enormous value to a unified voice so that general practice can be a peer at place or system level. It can provide a supportive web of services around the practice, so that the value of continuity and personal care can reach its full potential.
Primary care collaboratives
At-scale services could be effectively contracted through a primary care collaborative to be delivered by providers from across primary care.
Figure 1: One virtual organisation – one primary care collaborative
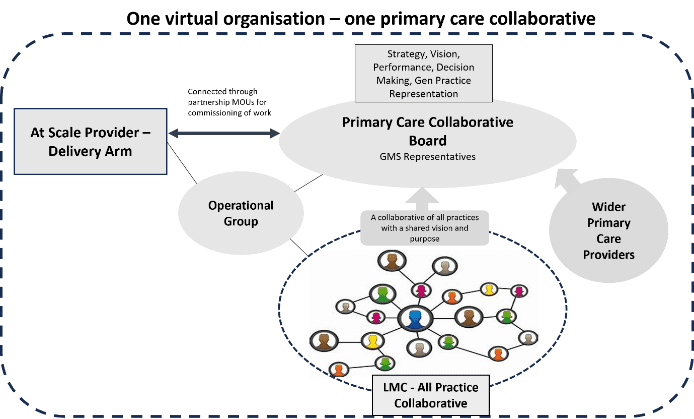
A functional primary care collaborative can provide:
- Reduced elective waiting lists.
- Improved urgent and emergency care by integrating 24/7 GP with other providers, to increase ability to hold risk out of hospital.
- Act as key integrator in neighbourhood health.
- Primary mental health care.
- Collaborative partnerships and alliance contracts with system partners primary, secondary care, VCSE, community and local authority.
- Stability to practices and a safety net for some practice risks.
- Centralised services, where it makes sense to do so, for the benefit of practices and providers, such as HR, finance, business intelligence and quality improvement.
Primary care is firmly located in the population that it serves and already demonstrates the ability to implement innovative services, efficiently and with the appropriate governance. This population-based approach aligns well with local authority partners. Likewise, when working as a collaborative, primary care is an effective peer to established NHS trusts. Many of the challenges affecting hospitals have solutions that sit or partly sit in the community, so this alignment is going to be particularly important.
Neighbourhood health
There is a government commitment to a new neighbourhood health service, and we need to make sure that at-scale general practice is ready to drive that transformation as it is well placed to be nimble and transformative.
General practice touches every part of the system and culturally understands the psychosocial factors that often are more important than those of a purely medical model. Partnerships with local authorities and VCSE are critical in building trust and engaging communities. Neighbourhood working cannot just be a diversion of the same work previously done in hospitals into the community, it must be about communities not services, and a change in mind set.
The culture is of one team wrapped around the patient, regardless of the employing organisation, and has taken strong transformational leadership from each organisation.
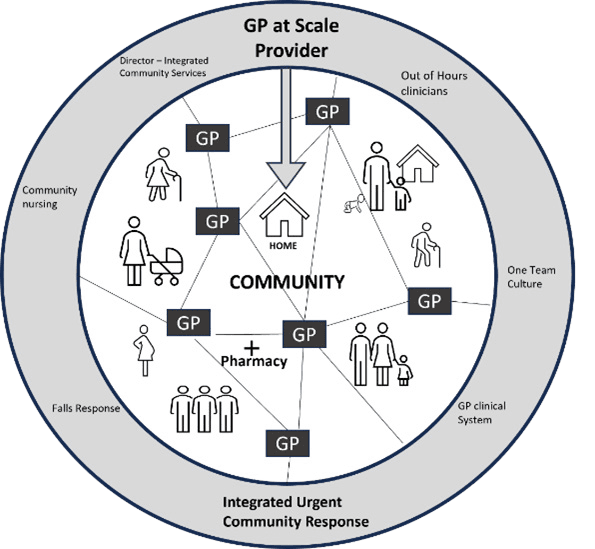
In Herefordshire, the at-scale GP provider (owned by all the practices) provides an integrated out-of-hospital emergency care service involving acute, community and GP assets, run 24/7. The culture is of one team wrapped around the patient, regardless of the employing organisation, and has taken strong transformational leadership from each organisation. Our at-scale GP provider has a joint appointment of one of its directors as the line manager of community services, which was truly a bold step by the trust involved. It has been highly effective in reducing unnecessary bureaucracy and making sure more time is spent on direct patient care. Our community services, urgent care teams, and out-of-hours clinicians all use the GP clinical system, so the GP has complete visibility and vice versa.
Figure 2: Herefordshire Urgent Community Care Model – wrap around the patient
There are a variety of potential organisational forms, but it may not be useful to define these as they have evolved locally depending on local strengths. They should, however, be united in the same unified principles and values:
- Rooted in NHS values.
- Aligned around a clear social purpose, reinvesting surplus into services and having transparency of operation.
- Have primary care values: valuing practice-based working, continuity when appropriate, and appropriate governance for the service.
- Collaborative in culture.
- Should be accountable to primary care.
- Should operate on a footprint that makes sense for place-based working.
- Should be shaped by local health needs and local populations should be at the heart of decision-making.
There is of course a ‘do nothing’ approach. If we take this approach, we may lose the opportunity to lead change. Local areas will need to decide collectively how they see service provision in their own area and which model enables the best bits of primary care to be preserved and provides the appropriate level of influence.
Conclusion
Change in the health service comes in cycles and we are entering a period of reform and transformation. In general practice, this may be a once in 20- year opportunity, with a new contract and similarly the rest of the NHS moving to a new operating model. Primary care collaboratives can drive the shift to neighbourhood working and, if resourced by the wider system, can move quickly to do so. It is now the time for place-based discussions at established forums and a wider discussion in practices and with primary care colleagues. The professions need to understand the opportunities and possible outcomes as larger partners are unlikely to wait.