
Unlocking reform and financial sustainability: NHS payment mechanisms for the integrated care age
Introduction: the drive for reform
Introduction: the drive for reform
The challenge of boosting productivity to meet growing demand
The NHS today faces considerable challenges. Improvements in life expectancy have stalled since 2010 and health inequalities have widened, exacerbated by the COVID-19 pandemic. [1] Around 7.75 million people are on the waiting list for planned treatment and waiting times continue to grow. [2] People are struggling to access primary care and waiting times for mental healthcare are similarly concerning. Staff are demoralised, as demonstrated by repeated industrial action and a fall in satisfaction in the latest NHS Staff Survey. [3]
The context for these challenges is not unique to the UK. Demand for healthcare services is continually rising disproportionate to the rest of the economy, primarily driven by an ageing population, as well as changing lifestyles, rising multi-morbidities and ever-evolving technologies enabling us to deliver more and more. [4] Today, nearly half of the UK population suffers from a long-term health condition, which will continue to consume a high proportion of healthcare expenditure. [5] Mental health conditions for children and young people are also rising. [6] The model of care envisaged when the NHS was founded in 1948 – of patients coming into hospital, receiving treatment, then going home healthy – is no longer the norm. At the same time, the scope of healthcare is continually expanding – from high-tech care for people with cancer to increasing medicalisation of common situations – and as such, so do public expectations of what the NHS should deliver.
As a result, demand for care is rising. For example, between 2010/11 and 2019/20, the number of hospital admissions rose approximately 16 per cent. [7] Overall GP consultations per registered patient per year for clinical staff groups rose from 4.29 in 2010/11 to 4.91 in 2014/15 and 5.66 in 2021/22. [8,9] By 2040, the number of people projected to be living with major illness in England is expected to rise to 9.1 million (2.5 million more than in 2019). [10] In an attempt to keep up with this, more and more money has been spent on healthcare – NHS expenditure has grown from £131.8 billion to £161.1 billion in 2010 to 2023/24 (equivalent to rising from 8 per cent to approximately 11 per cent of GDP). i
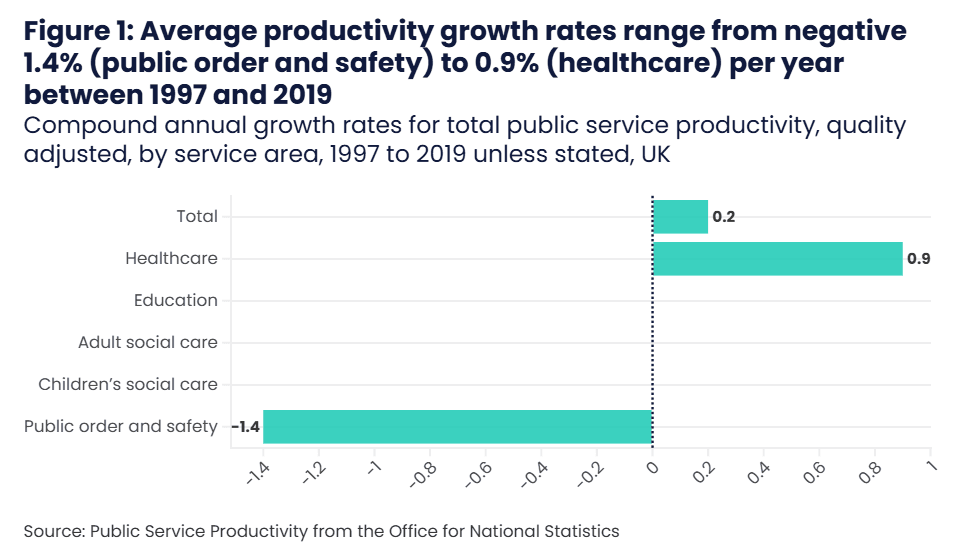
This growth in spend has corresponded with growth in the NHS workforce – between 2010 and 2023 staffing has increased by 315,000 full-time equivalent (FTE) staff (a 21 per cent increase). Much of this growth has been more recent, with an increase of 216,000 staff since 2019, (15 per cent). ii The rate of NHS productivity growth has averaged 0.9 per cent over the past 25 years, insufficient to keep pace. We should still note that healthcare productivity growth is higher than any other UK public sector services over the same time period. [11]
After rising for the previous two decades, overall productivity began falling by the end of the 2010s and has worsened following the COVID-19 pandemic. [12] Recent increases in staffing have often not translated into increases in volume of activity for many types of care. [13] However the extent of this is not fully clear as current measures of productivity capture volume rather than value of care, so falls in productivity growth are not as large as the data may suggest. Recent high inflation, particularly in energy and medicines prices, have contributed to a lower productivity figure. Nevertheless, significantly increasing productivity is therefore one of the greatest challenges facing the NHS. Improving healthcare productivity has a key role to play in lifting the UK’s overall productivity malaise.
Freedman and Wolf attribute lower productivity to: (a) the lack of capital investment for estate and digital infrastructure, which has made it harder to treat patients and caused inefficiencies; (b) high staff churn, more inexperienced staff and low staff morale; and (c) problems with hospital management and incentives from the centre. [14] This has been compounded by challenges with social care, with increasing numbers of people who are clinically fit for discharge remaining in hospital; the number of people who are in hospital facing delayed discharge has been above 20 per cent since January 2022. [15] There is also debate about whether growing regulatory demands are reducing the proportion of time spent on frontline delivery of care. Difficulties in increasing productivity can also be linked to the slow adoption of digital tools and technological solutions, as well as an outdated workforce model with limited incentives for delivery. However, evidence on the causes of recent NHS productivity trends is not fully clear.
The NHS Workforce Plan sets a target of between 1.5 per cent to 2 per cent annual NHS labour productivity increases over the coming decade, while the Health Foundation has estimated that funding for healthcare services would need to rise by 3.7-4.3 per cent to keep up with demand in the absence of productivity improvement – and public health, social care and health education funding by even higher rates. [16,17] For acute care services to keep up with rising demand indefinitely, without waiting times and waiting lists ever rising, would require an ever-growing share of national wealth being spent on health and care. [18] This is not sustainable.
Rather than just spending more money as revenue for day-to-day services and doing more of the same activity, the healthcare sector needs to do things differently and increase overall system effectiveness at keeping people healthier in the first place. Health and care leaders are conscious of the cost of inaction and look to plan services for the future, based on an understanding of the burden of disease in the long-term and not only the year ahead. This is not about changing how money is raised, but how it is spent.
The mission of integrated care systems
To reform how health and care services are provided and make the system more financially sustainable, parliament has created 42 integrated care systems (ICSs) in England. ICSs bring together all partners responsible for health and care, with integrated care boards (ICBs) responsible for commissioning NHS services. ICSs – as a collection of partners – have four core aims:
- improve outcomes in population health and healthcare,
- tackle inequalities in outcomes, experience and access,
- enhance productivity and value for money, and
- help the NHS support broader social and economic development. [19]
To achieve these goals, ICSs need to boost allocative efficiency – that is about spending money on services which improve health outcomes the most for every pound spent – by reducing demand for lower value-adding health care services and treatments in hospitals. This is strategically crucial to driving improvement and delivering better value given the pressures on the healthcare service. One of the ways of achieving this is to shift resources upstream towards primary and community care and earlier preventative interventions which in general, though not always, deliver better health value. By value in healthcare, we use the definition of ‘simultaneously the value delivered to the patient in the form of better health outcomes and the value delivered by the health system in terms of the most efficient use of society’s limited financial and other resources.’ [20]
If these services can prevent worsening ill health, they are a more efficient approach to improving health outcomes and limiting demand than more expensive downstream services. For instance, systems that invested more in community care saw 15 per cent lower non-elective admission rates and 10 per cent lower ambulance conveyance rates. [21,22] As a whole, a clinical intervention costs four times as much as a public health intervention, to add an extra year of healthy life, while 40 per cent of the burden on the NHS may be preventable through tackling the causes of avoidable chronic conditions. [23,24,25] Ensuring a healthy start to life through services for children and young people is also crucial to ensure they go on to have healthier lives as adults.
Crucially, this involves ICSs shifting their focus from just delivering healthcare to also taking responsibility, together with the patients, their family and communities, for improving health. Indeed, this was envisaged in the original 1946 Act that established the NHS, which defined the NHS’s roles as ‘a comprehensive health service designed to secure improvement in the physical and mental health of the people of England and Wales, and the prevention, diagnosis and treatment of disease.’ [26] Getting the best return on investment from preventative interventions will take some years and require some double running: meeting the healthcare demand from the population today, while preventing some of the demand for tomorrow. While preventative interventions are likely to reduce the rise in demand for healthcare services to lower than what it would otherwise be, demand is still likely to rise overall in any case.
It is therefore essential that ICSs also need to increase technical efficiency, delivering a higher volume and quality of activity in any setting at the lowest cost, to deliver timely, high-quality care for all patients. Much work has been done across the NHS to look at opportunities for greater technical efficiency – for example the productive ward work of NHSX’s Digital Productivity Programme and work carried out as part of the Getting it Right First Time (GIRFT) initiative. [27,28] Both found that improvements to core processes can significantly improve technical efficiency in a variety of settings. With most NHS spend in the acute sector, there are likely significant opportunities to improve overall NHS productivity and financial performance by boosting technical efficiency in acute providers. However, technical efficiency opportunities in primary and community care settings should not be overlooked and merit closer analysis. Price-setting is also an important nationally-led component of driving technical efficiency, supporting local efforts. [29]
Digital technologies and data analytics are now offering further opportunities to improve efficiency and effectiveness of care delivery. Analysis of population-level data, including from wearables that can provide a constant stream of real-time health data, can help to identify households with the greatest need and enable local services to reach out to avoid likely hospitalisation to improve allocative efficiency. Meanwhile, investment in basic technology and artificial intelligence (AI) can improve technical efficiency through automation. [30,31] Digital transcribing on ward rounds can save doctors valuable time on ward rounds. Use of wearables for health monitoring can reduce staff time for health checks on virtual wards. Every £1 spent on technology can generate £4 in savings from time which is freed up. [32] Improving both allocative and technical productivity at the same time is essential, but a significant challenge.
However, there are obstacles to ICSs delivering such changes which sit outside of their own power to fix. As ICS leaders set out in The State of Integrated Care Systems 2022/23: Riding the Storm, systems need from central government: [33]
- far greater freedom and influence over how money is spent to drive transformation in care
- greater capital funding to improve estate and digital infrastructure [34]
- a workforce fit for the future [35]
- a functioning social care market [36] and
- more local autonomy to deliver this reform.
These obstacles, and the opportunities which could be unlocked from addressing them, were addressed in the Rt Hon Patricia Hewitt’s review of ICSs, providing a blueprint for the future. [37] While not a new idea, the review also showed there is substantial consensus across the health and care sector for a fundamental shift from a model of treating ill health to preventing it in the first place – a view also supported by think tanks of different leanings. [38,39]
The role of payments and incentives
The Hewitt review also identified that ICSs need to deploy the right financial incentives to drive the change they want to achieve, as has been done in other countries and the UK historically, stating:
“Financial flows and payment mechanisms can play an important role in ensuring improved efficiency in care delivery… current approaches are not effective in driving value-based healthcare and while payment by results can help drive activity in a particular direction, it is important to recognise that it needs to be adopted in the context of wider system reform, incentivising prioritisation of resources on upstream activity.
“Many health systems in other parts of the world, including those that are entirely or largely taxpayer-funded, are developing payment models that support and incentivise a focus on health. Meanwhile, NHS funding remains over-focused on treatment of illness or injury rather than prevention of them and ICS partners struggle to work around over-complex, uncoordinated funding systems and rules in order to shift resource to where it is most needed. There are lessons from other systems that we should draw on.” [40]
The Hewitt review recommended that government and ICSs consider alternative payment mechanisms, “drawing upon international examples as well as local best practice, to identify most effective payment models to incentivise and enable better outcomes and significantly improve productivity.” In particular, this, according to the review, should consider: [41]
- incentives for individuals or communities to improve health behaviours
- an incentive payment-based model - providing payments to local care organisations (including social care and the VCFSE sector) to take on the management of people’s health and keep people out of hospital
- bundled payment models, which might generate a lead provider model covering costs across a whole pathway to drive an upstream shift in care and technical efficiency in provision at all levels
- payment by activity, where this is appropriate and is beneficial to drive value for populations.
Financial flows within the NHS are fragmented and work against integration. The different parts of the NHS, primary care, community care and hospital care are not financially incentivised to work better together. The financial system does not allow all partners within an ICS to benefit from returns from investments in another part of the system, disincentivising some cost-saving investments. Because the savings are in a different part of the financial system than the investment, ICSs are not able to invest to save and improve health while increasing their long-term financial sustainability. Given the separation of financial systems for the NHS and social care, this makes real integration of health and care services difficult.
To that end, this discussion paper considers learnings from the use of payment mechanisms in this country and internationally and makes three proposals for changing payments for healthcare services and incentives in integrated care systems. In doing so, it takes account of how payment mechanisms in different sectors of the NHS (such as primary, community, acute) interact with each other to shape the overall behaviour and performance of the NHS. The paper does not consider the prices paid for services under different payment mechanism options, noting that international analysis suggests that national price setting is an important driver of technical efficiency. [42] It also does not consider payments for individual NHS staff and the public, although these are areas which merit further exploration.
The paper aims to reflect honestly on the advantages and disadvantages of different payment mechanisms, recognising that there is rarely consensus in the sector on an ideal type. It is intended to be the start, not the end, of a conversation leading to more radical change over the next two to three years. ICSs – that is integrated care boards, NHS providers and other partners within systems – should work together to consider the best payment mechanisms for their local circumstances.
Methodology
The proposals, reflections and case studies in this report have been developed in consultation with an expert working group, made up of system and finance leads as well as subject matter experts, and in collaboration with KPMG. Adult social care, community and primary care stakeholders were also interviewed and engaged throughout the research process. Desk research and a literature review complemented the findings from the working group and stakeholder interviews.