
Pioneers of reform: realising a new vision of ICB strategic commissioning
How we get there: enablers for strategic commissioning
To bring about lasting reform, ICBs will need to convene system partners to, over time, make a decisive shift from contracting individual providers for activity (or services), towards contracting that drives collaboration to improve people’s health (or outcomes). For this work, we define strategic commissioning as:
‘The pursuit of the best possible health outcomes for a given population and experience for patients through the planning, purchasing, evaluation, integration and transformation of services, promotion of self-care and exercising system leadership to that end.’
At present, different stages of the NHS commissioning cycle can be illustrated as follows:
Before

After
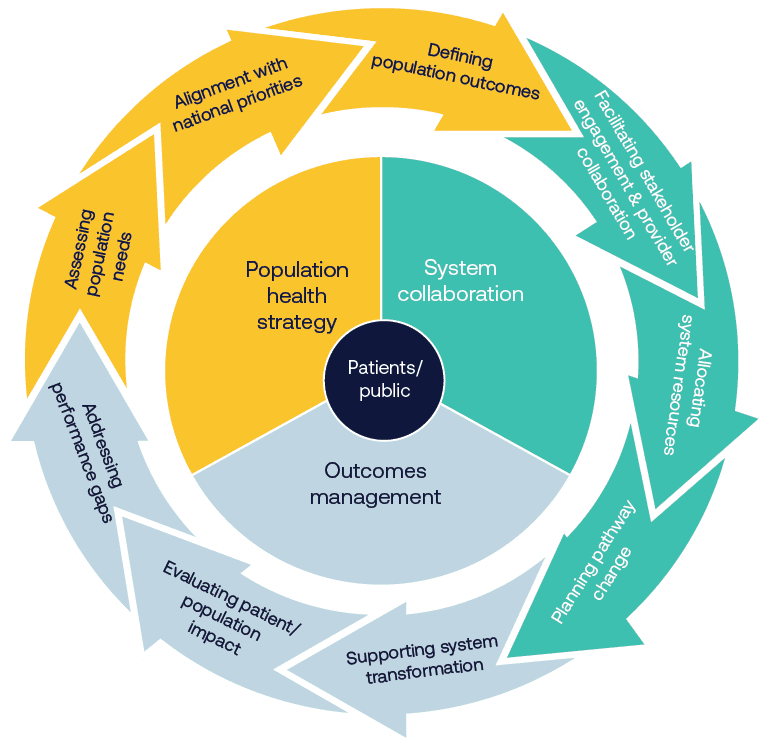
Joint forward-planning processes
Effective strategic commissioning requires robust population health planning. ICBs already undertake comprehensive population health needs assessments, using population health management systems and drawing on a rich array of data sources including public health data, hospital episode statistics, primary care data and social care metrics. Integrated care strategies are drawn from joint strategic needs assessments led by health and wellbeing boards. Quantitative analysis should be enriched by extensive community and stakeholder involvement to understand real local priorities, with particular attention paid to health inequalities and underserved populations.
These assessments will inform the development of specific, measurable population health outcomes across patient cohorts. Such outcomes span multiple domains: clinical metrics relating to disease progression such as diabetic complications; quality of life measures including improved mobility for elderly populations; system effects like reduced emergency admissions; and health equity metrics such as reduced variation in screening uptake. Each desired outcome will need to be accompanied by clear baseline metrics and should pinpoint the process improvements required, to provide a calibrated framework to measure progress and success.
If the ICP’s integrated care strategy sets the high-level outcomes system partners want to achieve, the ICB’s joint forward plan should set out how the ICB will allocate resources to achieve the NHS’s contribution to the integrated care strategy. Together, these strategies will form the basis for determining how and when resources need to be redeployed. Annual system plans constructed around the objectives declared will provide the concrete framework against which the contribution of all providers will be judged and rewarded. The timely publication of NHS England’s annual planning guidance and a streamlined approach to setting targets, such as the case for 2025/26, can support this planning process.
An enhanced incentive structure: payment mechanisms and tariffs
At present, commissioning processes are not geared towards influencing ways of working in operational delivery. Once funds have been committed to the detailed parameters set out in a provider’s contract, commissioners’ levers for change in real time tend to disappear. The actual deployment of resource becomes a matter for operational management. The dichotomy and binary nature of NHS contracting arrangements helped preserve stability when nascent systems were being established and while the driver of change was to incrementally improve standards of delivery and expand provision. But delivering the shifts outlined previously means rethinking our financial framework.
Currently, financial flows within the NHS are fragmented and work against integration. The different parts of the NHS – primary care, community care and hospital care – are not financially incentivised to work better together. The financial system does not allow all partners to benefit from returns on investments in another part of the system, disincentivising some quality-improving and cost-saving investments.
Payment by activity for acute elective care and block contracts elsewhere incentivises continuing flow of a greater share of NHS spending to later stage downstream interventions, rather than upstream where strategic commissioners want to shift resources. Paying for downstream activity based on demand and cost does little to improve value nor prevent that demand through earlier, cheaper intervention.
Different models should be explored that offer suitable and aligned incentive structures combining both financial and non-financial elements to encourage strong engagement and real commitment to improved outcomes. One option is to link baseline allocations to the portion of current budgets used to support provision formally designated as ‘essential services’. This could free up part of existing allocations so that they could help to offer additional outcome-based payments tied to the achievement of agreed population health goals. Monies not ‘earned’ under such arrangements would not be lost to the system, since shortfalls in one budget would be matched by uncommitted resources retained in another, but in the longer term funds would not continue to be distributed in such a way as to perpetuate failure or persistent shortfalls.
Contracting for specific health outcomes across a whole pathway for a specific patient cohort can help incentivise earlier and more cost-effective interventions, boosting allocative efficiency. However, this requires an appropriate ‘gain-share’ mechanism - or ‘loss-share’ mechanism if outcomes are not achieved – to ensure all system partners see a financial benefit and unite behind shared goals. Further information on existing models of outcomes-based commissioning and available options can be found in the NHS Confederation’s report, Unlocking Reform and Financial Sustainability: NHS Payment Mechanisms for the Integrated Care Age.
A shared savings model could similarly be used to reward achievement of population health outcomes that offered quantified ‘paybacks’. And specific incentives for reducing health inequalities might be a way of driving desired change, in the same way that service development funding monies have hitherto been used to secure particular service effects nationally. Locally, pooled budgets for shared priorities or matched funding arrangements for collaborative initiatives would be a natural extension of existing joint investment schemes.
Case study: Bundled payment system in the Netherlands
The Netherlands' bundled payment system for chronic conditions demonstrates how financial mechanisms can drive integration. The approach of single payments for complete care pathways led to improved diabetes care outcomes while reducing system fragmentation.
Alongside contracts, prices are also important. Current tariffs presume that the cost base of existing providers should provide a starting point for all decision-making. This approach perpetuates historical patterns of resource deployment and may no longer serve current needs. Once resources are committed to organisational budgets, their use can alter dramatically in-year. Length of stay can deteriorate, workforce changes may damage productivity, and overheads can increase without external scrutiny.
Two specific examples illustrate the challenges of current arrangements. Individual funding requests (IFRs) continue to consume commissioner time and resources despite the requisite clinical expertise – and all the commissioned resource - residing in providers. Similarly, out-of-area referrals often encourage providers to pass responsibility on to third parties rather than developing local solutions. These mechanisms need fundamental reform to support genuine system transformation.
System collaboration
To date, provider collaboratives have tended to operate within single sectors. For example, mental health provider collaboratives managing specialised commissioning budgets or acute provider collaboratives sharing clinical support services. These arrangements have demonstrated significant success in areas such as reducing out-of-area placements in mental health, standardising clinical practices, sharing workforce and delivering efficiencies through shared services.
Case study: East Midlands (IMPACT) Provider Collaborative
The East Midlands (IMPACT) Provider Collaborative for low and medium adult secure mental health services, led by Nottinghamshire Healthcare NHS Foundation Trust, consists of nine NHS and independent sector organisations. The IMPACT Provider Collaborative has a clinical model that seeks to transform adult secure care services across the East Midlands through improving patient pathways, the interfaces between the health, social care and criminal justice system, and ongoing service development. The collaborative has been able to reduce out-of-area placements from 20 per cent of patients to 5 per cent in 2023/2024.
However, strategic reform necessarily entails a significant evolution of how providers work together, extending collaboration beyond single sectors to encompass whole pathways of care. Achieving population health outcomes requires integration across the entire care journey, from primary care and community services through to acute care, mental health, social care, specialised services and the VCSE sector. This represents a step change in collaboration, to ensure shared accountability for the health outcomes defined in joint forward plans and integrated care strategies.
The successful elements of existing collaboratives - shared governance structures, risk-sharing arrangements, and operational protocols – can act as a springboard for extending them across traditional sectoral boundaries. For example, where mental health collaboratives have successfully reduced out-of-area placements through better coordination between mental health providers, this approach could expand to include primary care management of mental health, community-based crisis prevention, acute hospital liaison and social care support. Genuine end-to-end pathway integration would be supported by corresponding organisational and contractual mechanisms, with all providers sharing responsibility for specific results geared to producing desired population outcomes.
In this new model, providers collectively would have to align their resources to population health goals, rather than focusing separately on incremental improvements to services defined by their siloed funding envelopes. Clinicians and managers across the whole system would together take responsibility for pursuing broader outcomes. For instance, in managing population health for people with diabetes, primary care, community services, acute hospitals and mental health services would need to work in close partnership, sharing responsibility for everything from prevention and early intervention through to complex care management.
This evolutionary approach builds new elements into existing collaborative mechanisms by:
- extending successful governance models to encompass multi-sector partnerships
- creating shared accountability frameworks that span entire pathways
- developing integrated workforce models that enable staff to work flexibly across sector boundaries
- establishing shared clinical protocols that ensure consistent care delivery regardless of setting
- incentivising data and digital infrastructure that enables genuine population health management across all care settings.
The end goal is to create a model of system collaboration that matches the scope of the outcomes providers would together be responsible for achieving. One that moves from impressive but sector-specific improvements to genuine patient-focused transformation that can deliver the population health ambitions that ICBs are supposed to pioneer, and with a genuinely system-focused approach to performance management and oversight.
Oversight, accountability and performance management
Nationally, new mechanisms will be required to ensure mutual accountability for outcomes that will require the input and involvement of multiple organisations. As NHS England functions are brought back into the DHSC, further work is needed to ensure a clear delineation of functions between ICBs and the DHSC, including any new regional approach. This should build on the engagement and insights from the development of NHS England’s improvement and assurance framework.
NHS England previously signalled a change in its operating model that will see ICBs leading strategic commissioning and population health planning, while NHS England will assume responsibility for direct performance management of providers. ICBs will continue to have oversight of how providers deliver the outcomes that they have been commissioned to achieve for their population and need to build the requisite skills to do this. This ICB oversight role is essential to empower them to be pioneers of reform and to drive delivery of the three shifts. Providers’ statutory responsibilities for delivery, quality, safety and collaboration will be aligned in real time as never before. But for ICBs to oversee providers’ delivery of outcomes, they will also need to maintain the skills and expertise to oversee the quality and safety of services within the context of constrained management spend.
Performance monitoring is increasingly supported by real-time dashboards of key indicators, regular collaborative performance reviews and comprehensive tracking of patient experience and outcomes. Learning networks across provider collaboratives and systems can be used to facilitate continuous improvement, supported by best practice sharing forums and joint training programmes.
This includes the National Oversight and Assessment Framework (including ICB Capabilities Guidance, Performance, Improvement and Regulation Framework), and forthcoming updated NHS England Operating Framework and Strategic Commissioning Framework.
Risk management and success metrics
Effective risk management is integral to the success of this new way of working. Key risks around provider engagement, data quality, financial sustainability, workforce capacity and clinical safety will be actively managed as part of NHS England’s performance management regime. This will be done through early stakeholder engagement, development of shared processes, phased implementation approaches, joint workforce planning, and robust governance. The ICB’s role as a convenor that can take a system view will be particularly important.
Success can be measured both at system and operational levels. System-level metrics will track improvements in population health outcomes, reduction in health inequalities, value for money and patient experience. Operational metrics will focus on provider collaboration, quality standards, workforce satisfaction, service integration and financial performance. As much as possible, these should be streamlined and specific to support transformation and delivery to ensure leaders and staff have the headspace and time to deliver the changes needed.