
Pioneers of reform: realising a new vision of ICB strategic commissioning
Tomorrow’s vision: six shifts to strategic commissioning
Based on engagement with ICS leaders, the NHS Confederation proposes six shifts in behaviour that ICSs need to make to drive public service reform and ensure a sustainable health and care system for the future. NHS England’s forthcoming strategic commissioning framework provides an opportunity to set out detail and should align with the forthcoming ten-year plan for health, the NHS England operating model and other national policies to deliver this vision.
Our members see these shifts as key components of the wider cultural changes needed in the years ahead. As systems mature, these shifts will help move them towards a model of designing and commissioning services around population cohorts.
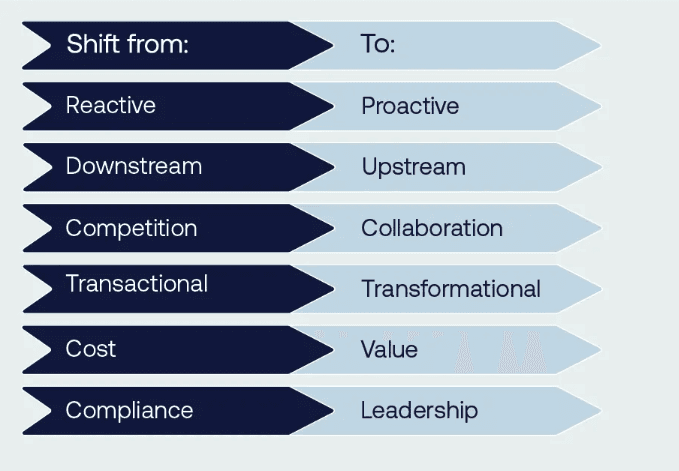
1. From reactive to proactive
The future of NHS commissioning must shift from managing demand to addressing the underlying needs of the population, tackling what Paul Corrigan described as the ‘curve of doom’: a widening gap between the growth in demand and provider capacity to supply care services. This transition requires moving beyond a reactive focus on pressures at the NHS ‘front door’ and instead embracing a more proactive and strategic approach. By using population segmentation to uncover hidden needs and opportunities, commissioners can better understand the diverse health requirements of different groups and target interventions accordingly. Data and analytics are central to this transformation, enabling the identification of trends, risks and areas for early intervention before pressures escalate.
Strategy development should be rooted in population insight, ensuring priorities are set based on the potential for the greatest impact. Healthcare utilisation management provides intelligence to inform resource allocation decisions that align capacity with actual needs. This approach ensures resources are deployed where they are most effective, reducing inefficiencies and addressing inequities across the system. Digital transformation will be critical in delivering this vision, empowering commissioners to work at system-wide levels and make data-driven decisions that optimise outcomes and ensure the NHS remains sustainable in the face of growing demand. To do so, system partners need to be able share data and access to patient records across different platforms.
Case study: North Central London's data-driven approach
North Central London ICB shows how sophisticated data analysis can transform commissioning decisions. The ICBs’s work on specialised services demonstrates the power of linking data across pathways. The system has brought together clinicians from across different settings to interpret complex data and propose new ways to address population needs. For example, their work on liver disease pathway redesign shows how data-driven insights can shape more preventative approaches to care, bringing together public health, population health staff, and clinicians from primary and secondary care.
Case study: Population cohort segmentation in Greater Manchester
Greater Manchester (GM) ICS provides healthcare for 3 million people living in ten places. As a system, GM has sought to improve population health while at the same time improving the financial position and service performance. To understand the health needs of the population, the ICS has used linked patient-level data and segmented the GM population to inform service and financial planning. Learning from Greater Manchester’s approach has been shared through via the NHS Confederation’s member forums and replicated by other ICSs.
2. From downstream to upstream
The future of NHS commissioning must prioritise a shift from downstream care, where ill health is treated as or when complications develop, and towards upstream, preventive measures that address the root causes of ill health. Prevention must take centre stage in commissioning decisions, ensuring that services are designed and funded to reduce the incidence of illness before it arises.
By supporting self-care and healthy lifestyle behaviours (primary prevention), the NHS can empower individuals to take greater control of their health, helping to reduce future demand on services. Early intervention also plays a crucial role in changing life trajectories, particularly by addressing risks and inequalities that, if left unaddressed, lead to more complex and costly care. Achieving this vision requires overcoming the significant barriers to prevention outlined in the NHS Confederation’s report, Unlocking Prevention in Integrated Care Systems, which explores the challenges and opportunities in embedding prevention within system-wide plans.
This upstream approach is underpinned by population health management, which uses data to identify trends and shape services around the needs of communities. Commissioners must increasingly look beyond traditional healthcare providers, recognising the value of community assets such as voluntary organisations, social networks, and local infrastructure, as part of the solution to improving health and wellbeing.
Primary and community care interventions, which prevent admissions to secondary care (secondary prevention), are also crucial. ICSs that invest more in community care have 15 per cent lower non-elective admission rates and 10 per cent lower ambulance conveyance rates. Every £1 spent on public health, primary and community care is correlated with £14 in gross value added to the economy.
To sustain this shift, investment should follow prevention opportunities, focusing resources on interventions with the potential to deliver long-term health benefits and alleviate pressure on the wider health and care system. Current approaches to measuring productivity are mostly limited to the acute sector and are activity based. Finding new ways to measure the benefits of shifting care and reducing more expensive activity will be crucial. A move from annual to multi-year planning cycles and allocations will help, as not all the benefits of prevention will be realisable over an annual cycle. Currently, high-value investments are sometimes deprioritised if they do not deliver a return in-year, ultimately perpetuating the financial challenges faced by ICSs.
3. From competition to collaboration
Sustainable system change depends fundamentally on strong relationships and shared objectives between partners. Technical solutions and structural changes alone cannot deliver transformation without the foundation of trust between organisations and professionals. In future, commissioning should facilitate a transition from competition between organisations to better collaboration across the health and care system. Although this will take time, joint mechanisms must replace organisational silos, enabling integrated working and fostering a culture of shared responsibility for outcomes.
Shared financial arrangements are critical to this shift, providing the foundation for collective action by aligning incentives and encouraging organisations to pool resources for the greater good. For example, a greater emphasis on a zero-based approach to spending or ‘open-book accounting’ could be explored. Performance standards must also evolve to operate seamlessly across boundaries, ensuring accountability and driving improvement in integrated service delivery across the system, not almost exclusively on acute sector activity.
This collaborative approach extends beyond the NHS, with social care and the third sector becoming equal partners in planning and delivering services. Initiatives such as the Better Care Fund should be geared toward realising the paybacks from pooled resources, allowing investment in services that reduce duplication and improve outcomes. Place-based partnerships are essential to driving integration at the local level, with Section 75 arrangements offering the legal and operational flexibility to support joint initiatives. The Provider Selection Regime (PSR) can enable a more co-ordinated and planned approach to procuring services. Together, these mechanisms create a framework for collaboration that moves away from transactional relationships, ensuring that the needs of patients and communities are placed at the heart of commissioning decisions.
Case study: Collaborative commissioning in Leicester, Leicestershire and Rutland
Leicester, Leicestershire and Rutland's integrated commissioning demonstrates how collaborative commissioning can work in practice. By implementing sophisticated pooled budget arrangements and joint commissioning approaches, they have moved beyond traditional organisational boundaries. The approach brings together health and social care resources through innovative risk-sharing agreements, enabling more flexible and responsive service delivery. This collaboration has proven particularly effective in areas like intermediate care and support for people with complex needs.
4. From transactional to transformational
A shift from a transactional to transformational approach is required to achieve sustainable improvements in health outcomes and system efficiency. Pathway commissioning, which focuses on the patient’s journey through services, must replace traditional organisation-based deals, to ensure care is designed and delivered holistically rather than fragmented by bureaucratic boundaries. Innovation will then drive decision-making across the system, embedding it as core business rather than allowing it to be treated as an optional add-on.
Transformational commissioning requires shared infrastructure to enable system-wide change and quality improvement initiatives that span organisational boundaries, fostering collaboration and integration. A stewardship model should empower staff and patients, giving them greater understanding of and influence in the way services are shaped and aligning care with the needs of the population. Additionally, long-term planning must take precedence over short-term, annual contracting cycles, to ensure that investments are aligned with strategic goals and that improvements are sustained over time. A forward-looking approach of this kind is essential to build a resilient health and care system capable of meeting the complex challenges that lie ahead.
Case study: HomeFirst in Leeds
The Leeds Health and Care Partnership’s HomeFirst Programme demonstrates how transformational partnership working can deliver tangible results. The partnership’s multi-agency HomeFirst Programme, developed through partnership between the council, integrated care board, NHS trusts, primary care and the voluntary and independent sector, has fundamentally redesigned intermediate care services. Rather than simply contracting for existing services, the system created a new person-centred, home-first model that spans organisational boundaries. The results speak to the power of this approach: 1,212 fewer adults a year admitted to hospital; a 36 per cent reduction in length of stay for people who no longer need to be in hospital requiring support on discharge; a 9.9-day reduction in short-term bed stays; and 607 more people returning home each year rather than being admitted to long-term care, compared to the baseline period.
5. From cost to value
The future of commissioning requires a more holistic approach to resource allocation, moving beyond traditional budgeting methods to ensure that funding is aligned with population needs and long-term health outcomes. Programme budgeting could help reflect the specific requirements of different population groups, enabling commissioners to direct resources where they are most needed. Pathway funding should replace siloed payment models, supporting integrated care and incentivising the transformation of services across entire patient journeys. Alongside these shifts, the adoption of new incentives such as blended or outcomes-based payments, will be critical in driving the delivery of more efficient and effective care.
Long-term and aligned financial planning between the NHS and local government is essential to create the space for transformative change, allowing organisations to invest in innovations that deliver paybacks over time. This philosophy must be underpinned by new productivity metrics that go beyond traditional efficiency measures, capturing the true value of care delivered across the system. Tools like an integration index, proposed in the 2019 NHS Long Term Plan but not yet operational, can measure what matters most, such as patient’s view of the care experience as well as outcomes and equity.
Commissioning decisions, including on medicines, should be factored in the downstream benefits of early intervention and prevention. The Provider Selection Regime also allows commissioners to make procurement decisions based on the overall return on their investment of public money, not just the lowest price. Together, these changes will support commissioners to make smarter, data-driven decisions that balance immediate pressures with long-term system sustainability.
Medicines are the most common healthcare intervention and second largest (and growing) area of NHS spend after staff. Optimising use of medicines is therefore essential to improving health outcomes, patient safety and value for money. In an ICS landscape, that medicines optimisation function needs 'systemisation', so it is better able to integrate activities across different providers and achieve better value for money, not just try to control costs. More progress is also needed to understand and manage the homecare medicines market, which could be an important driver of the shift from hospital to community care.
6. From compliance to leadership
Systems must evolve to empower leadership at all levels to drive sustainable improvement. Too often, overbearing instructions from the centre and risk aversion at a local level drives a culture within the NHS of compliance and looking upward for direction. Instead, policy should encourage and reward entrepreneurial leadership that looks outward for solutions, with greater risk appetite for doing things differently. Given the growing pressure on services, the overall risk of standing still outweighs the risk of change. However, the top-down compliance culture can mean that balance of risk for individual leaders can be the opposite.
Clinical leaders should play a central role in shaping system direction, using their expertise to guide strategic decisions and align services with patient needs. Frontline staff, empowered to influence priorities, will become instrumental in identifying issues early, proposing solutions, and ensuring care is grounded in real-world practice. Equally important is the participation of residents in service design, ensuring that those who rely on the NHS have a meaningful voice in shaping the future of healthcare delivery. ICBs’ chief medical officers and chief nursing officers embed clinical leadership on ICB boards, but clinical expertise in the provider sector should also be utilised to inform planning, particularly for provision of specialised services.
This distributed model of leadership encourages a greater appetite for risk and experimentation, underpinned by a cultural transformation that fosters innovation and continuous learning. Place-based leadership can then develop rapidly, enabling communities to respond flexibly to local challenges, while provider collaboratives will take on new roles that transcend traditional organisational boundaries. By dismantling existing hierarchies and nurturing a culture of shared responsibility, the NHS will move beyond compliance and embrace a leadership ethos capable of delivering better outcomes for all. Guidance and policy should focus on ‘what’ and ‘why’, leading ‘how’ to local determination.
Case study: Mid and South Essex's Stewardship Programme
Mid and South Essex exemplifies this shift toward distributed leadership through its innovative stewardship programme. Rather than maintaining traditional hierarchical controls, the system has developed a model where leadership responsibility is shared across multiple levels and organisations. The programme focuses on building capabilities among clinicians and managers to act as system stewards rather than just organisational leaders. This approach has enabled more rapid service transformation by empowering local decision-making while maintaining collective accountability for outcomes.