
Pioneers of reform: realising a new vision of ICB strategic commissioning
The case for change
Learning from the past
Following the purchaser-provider split in 1990, the early days of NHS commissioning were focused on increasing choice and tackling organisational inertia, which proved difficult to achieve. Separating commissioning from provision aimed to emphasise planning and allocating resources to meet population health needs.
Primary care trusts (PCTs), which operated as commissioning organisations between 2001 and 2013, demonstrated the benefits of working at scale. In some areas, PCTs achieved remarkable success by pooling expertise and resources, providing early examples of integrated working. These efforts showcased the potential of partnerships to address shared challenges and improve the public’s health.
However, PCTs often lacked formal mechanisms to align incentives and share risk across organisational boundaries, while separate accountability frameworks encouraged organisations to prioritise individual targets over system outcomes. This siloed approach ultimately constrained their ability to make change happen, as they were not able to coordinate action across the entire patient pathway.
Initiatives such as World Class Commissioning sought to make commissioning a highly skilled and outcomes-focused process. It introduced useful frameworks and methodologies but produced mixed results, highlighting the difficulty of nurturing new skills and capabilities without universal and sustained commitment to cultural change.
Clinical commissioning groups (CCGs) followed, after the Health and Care Act 2012. With clinical leadership on CCG boards, clinicians and managers developed strong partnerships that facilitated efforts to drive quality improvement. CCGs' boundaries and scale – co-terminous with local authorities – facilitated some integrated commissioning and provision of health and social care at the place level, using Section 75 agreements and structural integration through joint posts and committees.
CCGs began to develop some of the behaviours required for strategic commissioning. Despite the initial intention of the 2012 Act to increase competition, a pivot from competition to collaboration gradually emerged, first through sustainability and transformation partnerships, then non-statutory ICSs. Many CCGs had begun to take on the role of system convenor, managing competing provider interests and funding requests and looking to act in the interests of the whole population. However, their small scale inhibited this (regional providers, such as ambulance trusts, would have to work with up to 33 CCGs).
The Darzi review highlighted many valid drawbacks of the CCG model. But there were also three main benefits that ICBs inherited:
- Empowerment of clinical leadership and engagement
- Driving quality improvement.
- Facilitation of place-based integration.
This CCG legacy has, in some ways, set up ICBs well for the task of evolving how they commission. That said, the transition from CCGs to ICBs did, at least in the short-term, set back integration in some areas by unpicking good working relationships and pooled budgets at place level between CCGs and local authorities following the 2022 Act. ICSs are continuing to develop place-based leadership and devolve decision-making within systems. However, by ICS leaders’ own admission, the pace of devolution to place is slower than they have liked due to wider system pressures.
Today's reality: recent changes in commissioning policy
ICSs were ‘born into a storm’ in the wake of COVID-19 and austerity. The new structures require effective system working with providers remaining as sovereign organisations, albeit acquiring a new duty to have regard to the wider effect of their decisions and a duty to collaborate. ICSs extend beyond the 42 ICBs at their heart. Alongside each ICB are many other system partners, notably:
- local government
- NHS trusts and foundation trusts
- primary care providers
- social care providers
- the voluntary community and social enterprise (VCSE) sector
- universities and other public sector bodies
- other private sector partners.
Many of these partners come together to provide the strategic direction for the system through the integrated care partnership (ICP). ICBs and ICPs together acquired four core purposes. These are to:
- improve outcomes in population health and healthcare
- tackle inequalities in outcomes, experience and access
- enhance productivity and value for money
- help the NHS support broader social and economic development.
ICBs inherited most of their staff from CCGs, despite a different skill set being required in many areas. Only the most senior figures within ICBs (NEDs and board-level executives) were newly recruited. Some of these individuals transferred from CCGs, but others originated from elsewhere. Recruitment of new board-level leadership does not necessarily change culture and ways of working. Many ICB staff have moved across from the previous CCGs without the necessary development support to understand and adopt the new ways of working required for ICSs to succeed. Staff within ICBs, providers and across systems more widely need to shift attitudes and behaviours to achieve system working.
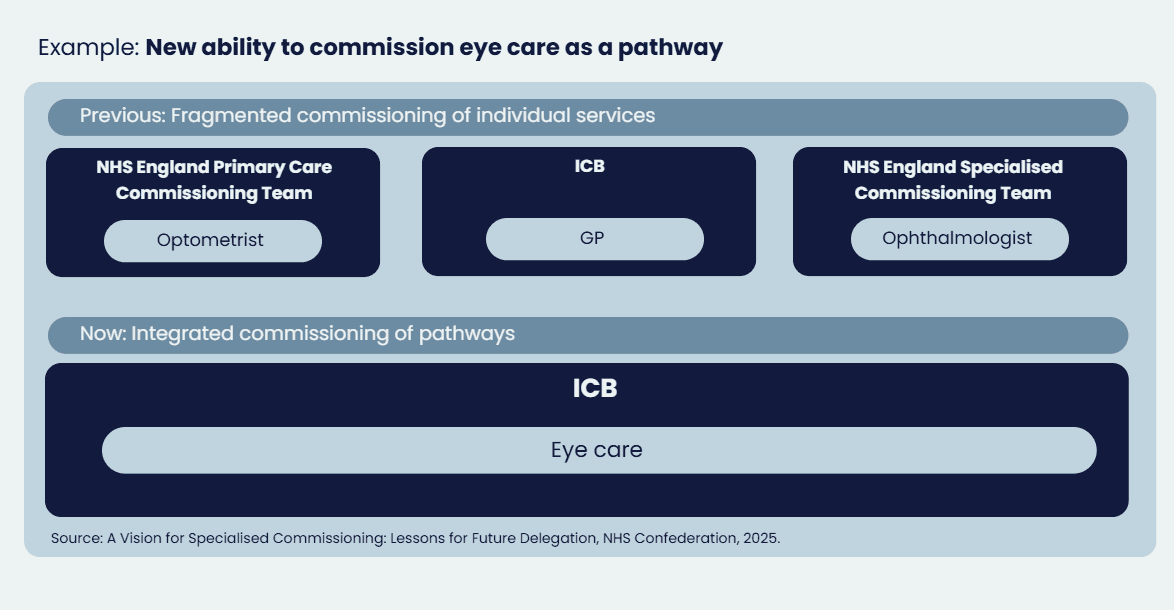
The delegation of additional commissioning responsibilities gives ICBs end-to-end commissioning of most care pathways, providing an opportunity to improve integration of care, access to services and help deliver care closer to home. The Darzi review highlighted the fragmentation of healthcare services resulting from the Health and Care Act 2012. As ICBs work at a larger footprint with a larger patient population, they can take on new functions previously sub-scale. Since 2022, NHS England is delegating several areas of commissioning to ICBs. This includes delegation of primary medical services, pharmacy, optometry and dental (POD) services, while the delegation of specialised service commissioning is underway, and vaccinations and screening commissioning responsibility will be transferred on 1 April 2026. This enables a wider change from commissioning individual providers to pathways of care, improving patient experience and delivering best value from available budgets.
Meanwhile, the operating environment for ICBs grows more challenging by the day. A 30 per cent reduction in Running Cost Allowance has forced organisational restructures, stretching leadership capacity and head space just as the agenda grows more complex. Place partnerships – crucial to delivering integrated care – are developing at markedly different speeds across the country, creating an uneven foundation for change.
Service and financial pressures are also making true collaboration harder. Despite the rhetoric of system working, block contracts and separate organisational budgets reinforce institutional boundaries. When targets and money present challenges, organisations understandably focus on their own imperatives rather than system priorities. This makes strategic commissioning more important than ever, but also more difficult to achieve. ICBs must work with their partners to drive transformation while tackling immediate pressures.
Transforming our health and care system
NHS contracting arrangements were designed originally to wrap around existing provider architecture and organisations’ baseline budgets, rather than around patients. Delivering the government’s reform agenda of three shifts – from hospital to community, from illness to prevention and from analogue to digital – requires changing commissioning. A new approach to commissioning and development of commissioning skills and expertise can help get patients the right care, at the right time in the right place, improving patients’ outcomes and experience. This includes shifting resources towards earlier intervention.
Provision of health and care is still too fragmented, to the detriment of patients’ outcomes and experiences. This fragmentation is reinforced by the many different funding streams that feed into the complex mosaic of statutory provision. Joining up these services is particularly important as more people are expected to be living with major illness and managing multiple long-term conditions, partly due to an ageing population. If real transformation and integration of services is to be accomplished, all partners must collaborate to make best use of their collective resource and improve patient care outcomes.
The cost of inaction is high; the public deserve a health and care system that is there for them in their time of need and contributes to the health and wealth of the nation. Strategic commissioning is at the heart of the transformation needed and must take a different starting point: the needs of populations, designing and commissioning services around the support and interventions residents require.